Laser treatment for fistula in ano-
A sphincter
saving approach
AETIOLOGY
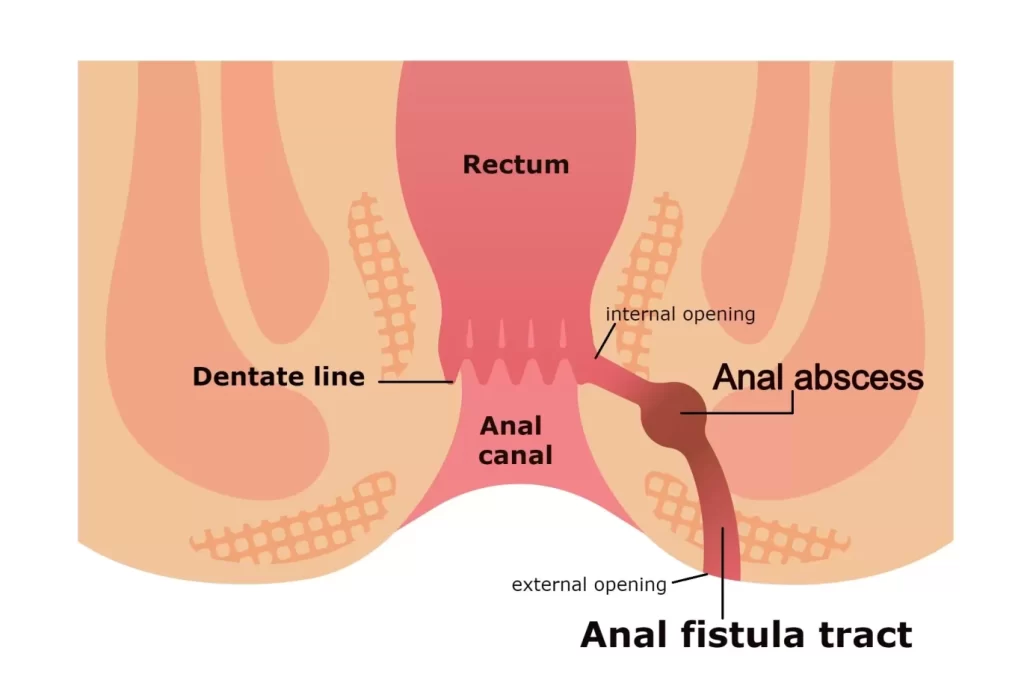
Infection of the crytoglandular glands extending to the intersphincteric space leading to abscess formation which ultimately drains into the perineum leading to a track lined by granulation tissue and epithelial cells with an inner and outer opening.
Secondery fistula- crohns, tb,lgv, trauma etc
FISTULA IN ANO
DEFFINITION : A fistula-in-ano is an abnormal hollow tract or cavity that is lined with granulation tissue and that connect a primary opening inside the anal canal to a secondary opening in the perianal skin. Secondary tracts may be multiple and can extend from the same primary opening
Energy causes shrinkage of the tissue and leading to the clouser of the tract.
Fiber is slowly withdrawn at 1mm/sec
10w-12w energy per second is usually delivered
Limited radial penetration depth (2-3mm beyond the fistula track)
WHETHER TO CLOSE THE INTERNAL OPENING?
Non closure
Mucosal advancement flap
Anodermal flap
NON CLOSURE OF THE INTERNAL OPENING
The FiLaC approach is designed to destroy both the crypt gland and the additional epithelial layer of the fistula track simultaneously by a photothermal effect with coincident obliteration of both the internal and external fistula orifices.
RECURRENCE RATE : Higher
EXPLANATION : The result of fistula re-opening with a linking up of the epithellal remnants of small undetected secondary tracks before the denaturaion effect of the laser can take effect.
DLPL-DISTAL LASER PROXIMAL LIGATION
1470nm /980nm DIODE LASER
600micron Radial Laser Emerging Fiber
Identifying The Tract And Inner Opening By Gentle Probing Or Hydrogen Peroxide
Dissecting The Tract In Between The External And Internal Sphincteric Plane
Ligating The Tract Near The Mucosa And Cutting It.
The rest of the tract was treated as per the Filac procedure.
CLOSURE OF THE INTERNAL OPENING
Recurrence Rate : Less
Preferred
Complicated Fistula
LITERATURE REVIEW
Primary Healing Rate 06.2%
Secondary Healing Rate 05.5%
Primary Healing Rate 71.4%
Primary Healing Rate : 81.8%
COMPLICATIONS
IMMEDIATE : BLEEDING BURN
DELAYED : INCONTINENCE FAILURE OF CLOSURE ABSCESS FORMATION
COMPARING DLPL AND FILAC
DLPL
For Complex Fistula
Dissection Of The Intersphincteric Plane Required
If Interspincteric Absess is Present It Gets Drained
Recurrence Rate Is 5%
No Sphincter Injury
DLPL
For Straight Fistulous Tract
No Such Dissection Required
No Drainage
Recurrence Rate Is 15%
Quicker Post Op Recovery
No Sphincter Injury
LASER AS AN IMPORTANT TOOL FOR PROCTOLOGIST
LASERS provide newer treatment options.
providing faster recovery.
Lesser pain.
Better outcome of surgery.
Smaller wounds
Making proctology a day care procedure
HAEMORRHOIDS
World wide prevalence from 2.9% to 27.9%
Men more the females
Effects at middle age
The anorectal vascular cushions along with the internal anal sphincter are essential in the maintainence of continence by providing soft tissue support and keeping the anal canal closed tightly.
There are typically three major anal cushions , located in the right anterior, right posterior and left lateral aspect of the anal canal and various numbers of minor cushions lying between them
GRADATION OF HAEMORRHOIDS
Internal Hamerrhold Grades
No prolapse, just prominent blood vessels
Prolapse upon bearing down, but spontaneous reduction
Prolapse upon bearing down requiring manual reduction